
Standerwick et al. [62] suggest a further, complementary model of craniofacial growth.
According to this model, the rotation and growth of the brain influence the superficial musculoaponeurotic systems of the face, on account of the tension of the occipitofrontal muscles and associated fascia.
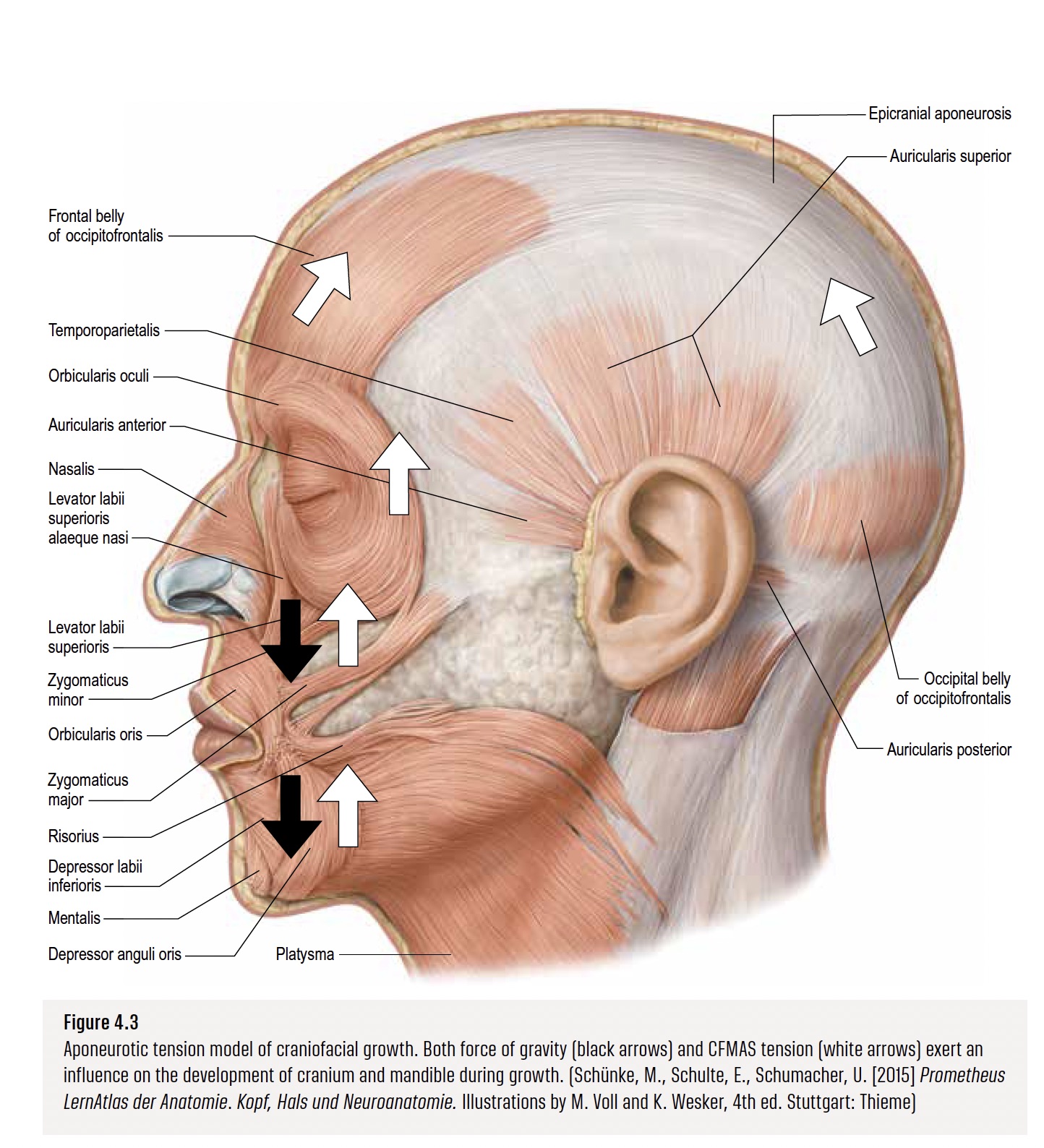
By means of this the craniofacial musculoaponeurotic system (CFMAS) of the cranium has a direct effect on the development of the maxilla and mandible.
It forms the basis of the aponeurotic tension model of craniofacial growth.
Some aspects of this model are further explained below, supplemented with examples from the literature.
Via the CFMAS, cranial rotation has an effect on the expression of face shape.
Tension of the CFMAS not only exerts dorsal, restrictive pressure, but also results in relative cranial tension.
This can have an anabolic effect on growth.
It is counterbalanced by the craniocaudal tension of the suprahyoid muscles, which have a connection with the growth of the cervical vertebrae via their attachments ([48], [50]).
Genetic factors such as short or long head shape affect the CFMAS and can influence maxillomandibular rotation.
CFMAS tension significantly depends on resting muscle tone and suppleness of the connective tissue, and it is greater in broad (leptoprosopic) than in narrow (euryprosopic) faces, on account of their different muscle morphologies ([47], [48]).
The effects of gravity on the viscerocranium are modified by the CFMAS, because muscle growth increases during puberty, along with a densification of the associated connective tissue components.
This resistance of the CFMAS relative to the effects of gravity results in an anterior displacement of the mid-face brought about through maxillary contact with the lower jaw and functional occlusion of the teeth.
This divergence of the facial planes in combination with the opposing forces of gravity and of the CFMAS appear to have a wedge effect (Fig. 4.1).
As a result, leptoprosopic facial types with a hyperdivergent angle of the mandibular plane normally have an upper jaw that is retrusive in the sagittal direction.

According to this model, the pivot for the rotation of the lower jaw is the pterygomasseteric sling, formed by the aponeuroses of the masseter and medial pterygoid muscles at the angle of the mandible [23].
The pterygomasseteric sling is seen as the original neonatal site of muscle accumulation that approximates the neutral zone of the mandibular periosteal sleeve, where little periosteal migration occurs [26].
The CFMAS reaches the anterior part of the lower jaw via the modiolus and osteocutaneous ligaments (Fig. 4.3).
This causes anticlockwise, forward maxillomandibular rotation ([8], [9]), which brings about a separation of the articular surfaces of the temporomandibular joint, producing a caudad movement of the mandibular angle and raised position of the ramus relative to the anterior height of the face.

In dolichocephaly (long head shape), bite force is often reduced, and there is clockwise, backward maxillomandibular rotation; this may be due to reduced CFMAS tension.
Airway obstructions often occur in these individuals, leading to a forward position of the tongue (relative to the pterygomasseteric sling), as a result of which the gravitational effects predominate over the CFMAS effects [18].
This in turn leads to more marked clockwise rotation of the lower jaw, to a narrow, longer face and backward rotation of the nose (dorsal hump).
Since there is clockwise rotation around the pterygomasseteric sling, the ramus too does not move dorsally (relative to the pterygomasseteric sling), creating a greater likelihood of tooth crowding.
Fig.
4.4 sets out the modulation of brain growth by cranial rotation and CFMAS tension in the form of an algorithm.
Brain growth proceeds both during normal development and consequent to trauma (concussion, drug use) in temporary regional growth spurts.
CFMAS tension is influenced by cranial rotation and by the development of the brain and postural control, and CFMAS tension is manifested as a weak or strong phenotype displaying a maxillo-mandibular rotation in the clockwise or anticlockwise direction respectively.
There is also increased overbite and progressive limitation of the mandibular dento-alveolar complex [10].

Check Liem 2023




